On April 19, 2011, the "Proposed Statement of Antitrust Enforcement Policy Regarding Accountable Care Organizations Participating in the Medicare Shared Savings Program" ("Proposed Statement") was published in the Federal Register.[1] The public was given the opportunity to submit comments regarding the Proposed Statement by May 31, 2011.
The Proposed Statement protects Medicare-approved accountable care organizations ("ACOs") participating in the Medicare Shared Savings Program ("MSSP") from per se enforcement of the antitrust laws and establishes criteria for evaluating an ACO's risk of an antitrust law challenge from the Federal Trade Commission ("FTC") and the Department of Justice ("DOJ") under a "rule of reason" analysis. Among the criteria used to evaluate an ACO's risk of an antitrust challenge is the ACO applicant's "market share" within each of its service lines. The market share is a measure of the share of services an ACO participant provides in its Primary Service Area ("PSA") relative to other providers. The share of services that each ACO participant provides in its PSA — which is referred to as the participant's "PSA share" — is the key factor that the agencies are proposing to use for determining whether an ACO will receive "Safety Zone" protection from the antitrust laws or be subject to mandatory expedited review from the agencies in order to participate in the MSSP. Consequently, most organizations that are considering forming ACOs will need to calculate the PSA shares of their participant-providers.
On May 9, 2011, the FTC and DOJ held a panel discussion to understand what concerns the public may have with the Proposed Statement. During that discussion, the agencies seemed open to the idea of slightly modifying the PSA share calculations described below, although it was clear that a market assessment that may have many of the characteristics described below would still be required. Therefore, while the FTC and DOJ may modify the Proposed Statement in response to public comments, the market assessment is likely to have many of the characteristics of the Proposed Statement.
We have provided in this alert a "step-by-step" description of the proposed method, as well as an illustration, for calculating PSA shares.
A. Identification of All Service Categories
Each ACO participant must determine the specific service categories that it offers based on a service category classification scheme described in the Proposed Statement. Categories for inpatient services are based on "Medicare Care Specialty Codes" ("MDCs"), categories for outpatient facility services are based on Centers for Medicare & Medicaid Services ("CMS")-defined outpatient categories. Categories for physician services are based on CMS Medicare Specialty Codes ("MSCs") that reflect the specialty designated on a physician's Medicare Enrollment Application. According to the Proposed Statement, CMS will be making lists of the categories in each of these service classes (inpatient, outpatient, and physician services) publicly available.
B. Identification of PSAs
The PSA for each service category provided by an ACO participant is defined as the "lowest number of contiguous zip codes from which the ACO participant draws at least 75% of it patients" for that particular service category. Therefore, to identify PSAs, an ACO participant will need to quantify the number of patients it sees from each zip code.
| Note that the Proposed Statement does not specify the time period that ACO participants should use for quantifying the number of patients seen from each zip code. Maintaining consistency with PSA share measurements, described below, would require calculations to be made based on service encounters during the most recent calendar year. |
C. Identification of the ACO Participants and Service Categories that Should Calculate PSA Share(s)
There are two circumstances in which the PSA share of an ACO participant can directly affect an ACO's antitrust risk classification under the Proposed Statement:
- If two or more ACO participants provide a common category of service(s) within a particular PSA, the PSA shares of these two ACO participants for that common category of service(s) will directly impact whether the ACO falls within the Safety Zone or requires expedited review from the agencies in order to participate in the MSSP. For example, if Cardiology Group A provides cardiology services in the PSA of Cardiology Group B, both groups will have to calculate their combined share of cardiology services in Group B's PSA. Similarly, if Group B provides cardiology services in Group A's PSA, the groups will have to calculate their combined share in Group A's PSA.
| Note that for two ACO participants to share a common category of service(s) within a particular PSA, the PSAs of the participants do not need to overlap. Two ACO participants will share a common service category if the PSA of one ACO participant overlaps with the geographic service area of another ACO participant (i.e.,Participant A sees patients from Participant B's PSA). This concept is illustrated in the diagram at the end of this alert. |
- If an ACO participant suspects that it might be a "dominant provider" in its PSA,a PSA calculation is necessary to determine whether the ACO is, in fact, a dominant provider. To be a dominant provider, an ACO participant must have a PSA share of greater than 50 percent for a particular service category and be the only ACO participant providing that service in its PSA. Because the market share for physicians and for outpatient services is based on Medicare fee-for-service revenue, potential participants may want to consider whether they think their Medicare fee-for-service volume is higher than their competitors' volumes.
D. Calculation of the PSA Share
The Proposed Statement establishes three different methods for calculating PSA share based on whether the service is classified as an inpatient, an outpatient, or a physician service. Each method of calculation has a similar underlying approach: the ACO must determine the "quantity" of services in a particular service category that residents in the PSA received from its providers and divide this value by the total "quantity" of services in that service category that residents in the PSA received cumulatively from all providers.
The Proposed Statement defines the metrics that ACOs must use to determine the "quantity" of services that PSA residents receive from ACO participants and cumulatively from all providers.
Calculations for Physicians' Services. For services classified as "physician services," the ACO must use "Medicare fee-for-service allowed charges" within the most recent calendar year. CMS is going to make that information publicly available. To determine the market share, the ACO participants must pool the allowed charges for any common service provided by ACO participants in a participant's PSA. That number is the numerator. The denominator is the total fee-for-service-allowed charges for all physicians in that PSA. For services rarely used by Medicare beneficiaries, such as obstetric and pediatric services, the Proposed Statement allows ACOs to use other available data to calculate PSA shares.
| The FTC and DOJ understand that such calculations may be difficult for physician groups, and are taking alternative approaches under advisement. |
Calculations for Outpatient Services. For services classified as "outpatient" services, the ACO must use "Medicare fee-for-service payments" within the most recent calendar year. As above, to determine the market share, the ACO participants must pool the allowed charges for any common outpatient service provided by an ACO participant in a participant's PSA. That number is the numerator. The denominator is the total fee-for-service-allowed charges for the service for all physicians in that PSA.
Calculations for Inpatient Hospital Services. For services classified as "inpatient" services, the ACO must use discharge data from the most recent year that state-level all-payer hospital discharge data is available. If the state does not have such data available, the ACO must use Medicare fee-for-service payment data (which will be made available by CMS, when necessary).
| Note that applying the above-described metrics for calculating the PSA shares of physician and outpatient services produces a PSA share value that reflects only an ACO's relative share of service to Medicare beneficiaries. Therefore, depending on a provider's case mix, the PSA share values for physician and outpatient services may not be representative of the provider's actual PSA "market share." Recognizing this possible divergence between PSA share and overall market share within a PSA, the Proposed Statement requires an applicant ACO subject to mandatory expedited review from the agencies (i.e., an ACO with participating providers that have greater than a 50-percent PSA share) to provide information relating to its market share in the commercial market if its Medicare PSA share diverges from its non-Medicare PSA share. In such cases, the ACO applicant must submit with its expedited review application both its standard PSA share calculations and comparable PSA calculations for each common service provided to commercial customers. |
Quick Reference Guide for Key Terms
| Proposed Statement Term | Definition | Where Is This Information Available? |
|---|---|---|
| PSA | A PSA (or Primary Service Area) is the lowest number of contiguous zip codes from which the ACO participant draws at least 75 percent of its patients for a particular service category. | Providers will need to use their own data to determine PSAs. |
| MDC | An MDC (or Major Diagnostic Category) is an inpatient service category (e.g., MDC 5 refers to services related to diseases and disorders of the circulatory system). | CMS will make publicly available the most current list of MDCs. |
| MSC | An MSC (or Medicare Specialty Code) is a CMS-defined specialty category for physician services (e.g., MSC 20 refers to an orthopedic surgery specialty). | CMS will make publicly available the most current list of applicable MSCs. |
| Medicare-Allowed Charges | This term means the amount of charges a provider is entitled to receive from the Medicare program for a service provided during the most recent calendar year for which such data is available. | CMS will make publicly available the data necessary to calculate aggregate Medicare allowed charges for each service, by zip code. http://www.cms.gov/apps/files/aco/application-zipcodes.zip. |
| Medicare fee-for-service payments for PSAs | This term means the payment amount a provider received from the Medicare Program for a particular service provided during the most recent calendar year for which such data is available. | CMS will make publicly available the data necessary to calculate aggregate Medicare-allowed payments for each service, by zip code. That data is available at http://www.cms.gov/apps/files/aco/application-zipcodes.zip. |
| Discharge Data | This term refers to state-level all-payer hospital discharge data for the most recent calendar year for which data is available. | Discharge data is only available in some states. |
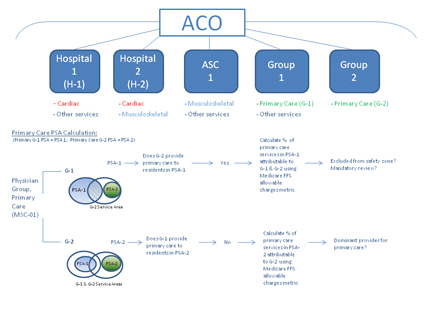
Process for Calculating PSA Shares
The diagram below is an illustration of the process for calculating PSA shares for primary care services in a hypothetical ACO in which two ACO participants provide primary care services in overlapping geographic areas.
For more information about this issue of IMPLEMENTING HEALTH AND INSURANCE REFORM, please contact one of the authors below or the member of the firm who normally handles your legal matters.
| Patricia M. Wagner Member Epstein Becker Green Washington, DC 202/861-4182 pwagner@ebglaw.com |
Ross K. Friedberg Associate Epstein Becker Green Washington, DC 202/861-0900 |
ENDNOTE
[1] 76 Fed. Reg. 21894 (April 19, 2011).
Resources
People
 General Counsel / Chief Privacy Officer
General Counsel / Chief Privacy Officer